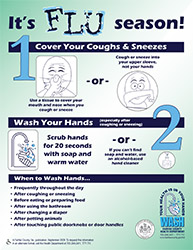
Influenza, also known as the flu, is a highly contagious respiratory infection caused by flu viruses. The respiratory system is the parts of your body that help you breathe.
Seasonal flu is caused by viruses that already circulate among people. While seasonal flu viruses are detected year-round, in the United States flu season usually starts in late fall and lasts throughout the winter, sometimes into early spring. Most people have some immunity and a vaccine is available to help prevent the flu.
CDC estimates that between 140,000 – 710,000 hospitalizations and 12,000 – 52,000 deaths occurred annually between 2010 and 2020.
There is more than one type of flu. Other types of flu include:
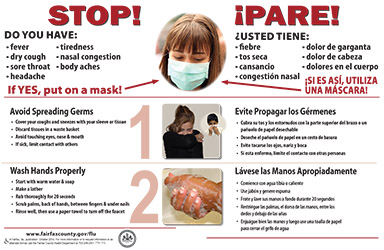
Flu, the common cold, and COVID-19 are all contagious respiratory illnesses, but they are caused by different viruses. You cannot tell the difference between flu and COVID-19 by the symptoms alone because they have some of the same signs and symptoms. Specific testing is needed to tell what the illness is.


 Influenza, known as the flu, is a highly contagious infection of the breathing system (nose, throat and lungs) caused by flu viruses.
Influenza, known as the flu, is a highly contagious infection of the breathing system (nose, throat and lungs) caused by flu viruses.